561.391.1728
SNeedell@bocaradiology.com
www.bocaradiology.com
For purposes of MR imaging, the foot is divided into three exams:
1. Ankle/Hindfoot/Midfoot (everything behind metatarsals)
2. Midfoot (neck of calcaneus thru metatarsals) - same as forefoot protocol but centered over midfoot
3. Forefoot/toes (metatarsals & toes)
MRIs for tendons & ligaments use "Ankle" protocol unless AOI is specifically in the forefoot.
"Foot" MRIs should be treated as Ankle/Hindfoot/Midfoot MRIs until proven otherwise.
Exceptions : For neuroma, mass, stress fracture,
or osteomyelitis in the forefoot- do a dedicated forefoot (metatarsals and toes) exam.
Plantar fibroma & LisFranc fractures- use dedicated midfoot protocol.
- only image one foot at a time
Sagittal T1 & STIR
Axial PD & fat sat T2 (or T2 without fat sat if low field)
Coronal PD
-Ankle tendons and ligaments are best imaged with the foot plantar flexed 15-30°. So avoid using the chimney in a coil. Position the calcaneus in the middle of the coil and the relaxed foot will fit comfortably in the coil at the correct degree of plantar flexion.
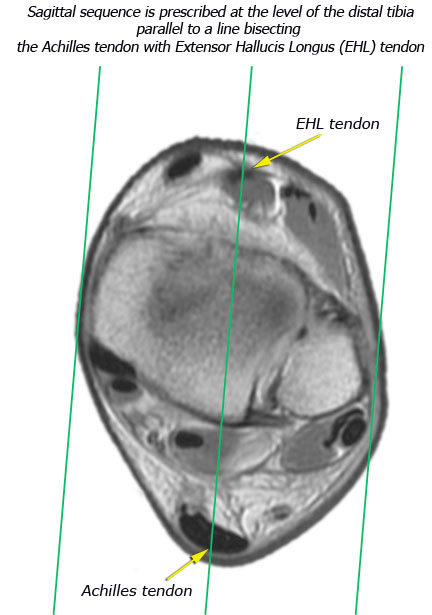
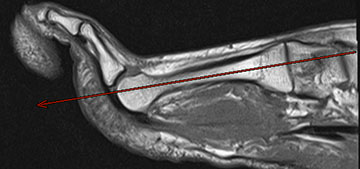
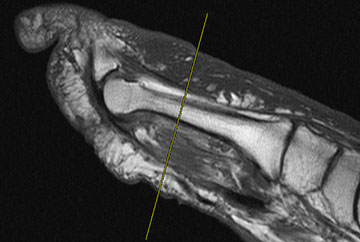
- Sagittal sequence is prescribed off an axial scout at the level of the distal tibia (see figure below) parallel to a line bisecting the Achilles tendon with the Extensor Hallucis Longus (EHL) tendon. If you have trouble identifying the EHL tendon, then scroll inferiorly and use the 2nd metatarsal as your inferior landmark.
-Inferiorly, axial sections through the ankle should include the fifth metatarsal base.
-Superiorly, axial images should include about 3 cm above the level of the ankle joint. If the exam is specifically to evaluate the Achilles tendon, make sure sagittal and axial images include the Achilles myotendinous junction.
-Angle axials tangential to distal tibia (see figure below).

LONGITUDINAL (long axis)

TRANSVERSE (short axis) at level of MTP joint
- Place patient prone to image forefoot whenever possible, especially when evaluating for Morton's neuroma.
- Look at the sagittal or longitudinal STIR images before you prescribe the transverse sections so that you can be sure you've covered all the pathology (bright signal on STIR = edema = pathology).
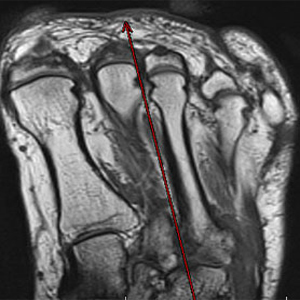
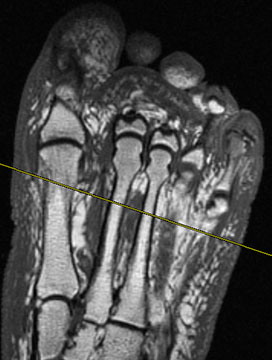
- Forefoot images should be prescribed off a short axis scout at the level of the MTP joints.
- Always mark region of concern with a Vitamin E or fish oil tablet.
- Use small FOVs
Longitudinal T1 (1mm) & STIR (3/0.5mm)
Transverse T1 & STIR (4/1 mm)
Sagittal PD (or T1 if to evaluate infection) & STIR (4/1 mm)
If the patient has had prior neuroma surgery then add a transverse post gad T1W (with fat sat if available)
Plantar fibroma & LisFranc fractures of midfoot
If the area of concern is isolated to the midfoot, such as plantar fibroma, then center the coil over the area of interest & use forefoot protocol.
MATRIX:
If you have enough signal, use 512 x 256 for T1W sequences. STIR & T2 fat sat can be 256x192.


ADA Compliance Policy: In accordance with the American with Disabilities Act, Boca Radiology Group strives to ensure that our web site is accessible to individuals with disabilities. If you have any questions or suggestions regarding the accessibility of this site, please contact us via email or call us at 561.391.1728, so we can ensure you receive the information you are seeking.
© 2023 All Rights Reserved